Brain & Skull Base Tumors
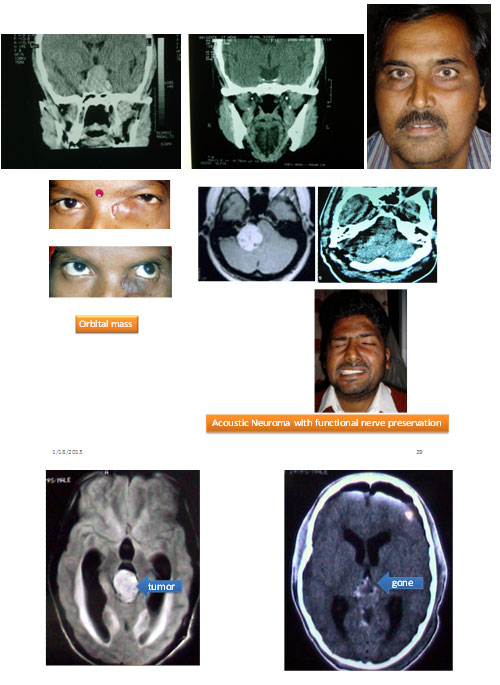
We operate all types of tumors in any location including Brain, spine, orbit, Skull Base and nerves. We use microsurgery or endoscopic surgery for all cases, both benign & malignant.
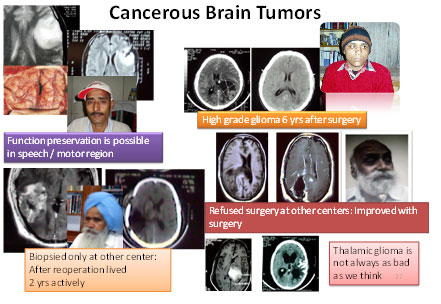
Brain tumor present with raised ICP, focal deficit, seizure, global deficit, psychiatric symptoms. They can be Benign/Malignant, Disseminated/solitary, Localized / Diffuse, Contained / Infiltrating. There are no stages and generally do not spread outside cranium.
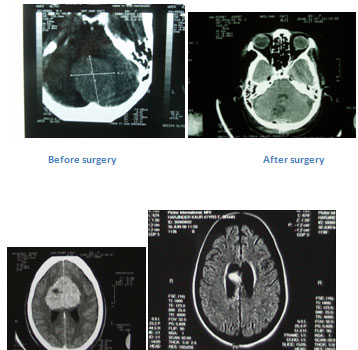
Surgery remains the mainstay of treatment for most of tumors. Complete tumor removal have been possible in most of our cases without the need of Neuronavigation or intraoperative MRI or CT (very costly tools and possibly not much needed), which was always confirmed on CT or MRI after surgery. Preservation of functions by intraoperative neurophysiological monitoring, awake craniotomy or special approaches are used in special cases with desired benefits. We use gamma knife or X-knife only for small invincible lesions.
Almost always complete tumor removal through safest corridor, for even operated or rejected cases has given good results. At our center, no age or functional status is absolute contraindication to surgery. Similar good results can be achieved at any age.
Pituitary tumors
We remove them through Transnasal Transhphenoidal route with the help of Microscope for 14 years or Endoscope for 10 years. In microsurgicval approach cut is needed behind lip or inside the nose. In endoscopic approach no cut is made outside. We confirm the tumor complete tumour removal by MRI or CT scan within 1-2 days after surgery and within 3-6 months after that. Increase in urine production (Diabetes Insipidus) used to occur after surgery for few days to weeks; Now it does not occur more than few hour to 1-2 day. No patient had it persisted permanently. One of patient had worsening in pituitary controlled hormonal level as compared to before surgery status in earlier cases. However, for last many cases even transient worsening is not seen in almost all cases. Most of the cases present with worsening of eyesight which invariably improves in all cases but may no trecover permanently. Most of the patients are satisfied with the results and outcome. CSF leak has been the biggest challenge, we lost few patients because of CSF (brain-fluid) leak associated infection; however, for last many years, no patient had problematic CSF leak.
We have operated two patients even during pregnancy saving child as well as the eyesight of the mother successfully.
Open method by opening head was never required in last 12 years or so
Colloid Cyst third ventricle
Colloid Cyst third ventricle is removed completely with help of endoscope or microsurgical approach.
Glomus jugulare, Meningiomas
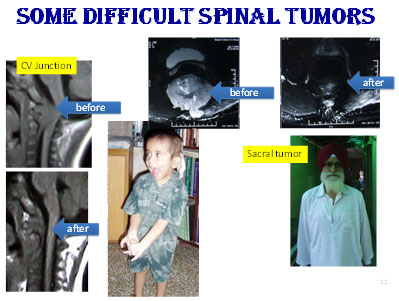
Spinal Tumours
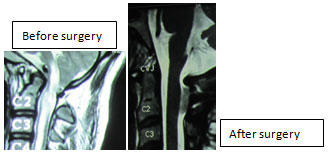
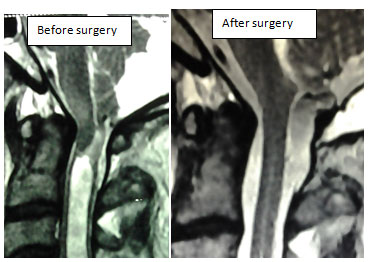
We excise all types of Extradural, Intradural extramedullary and Intramedullary tumours. Most of the cases have significant clinical recovery. We completely removed cervical intramedullary tumors in all cases except in one low Grade glioma: , no one required even ventilator support after surgery, no one deteriorated from before surgery status, all improved except one who was given radiotherapy by his physician although he maintained ambulatory status.
We have applied minimally invasive techniques in some of our cases with success.
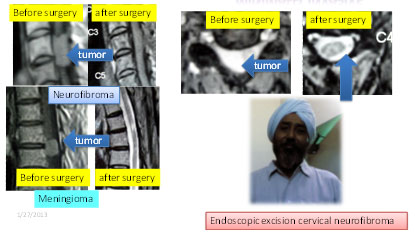 New technique for removal of spinal tumour without opening up the spine in Single approach: Worldwide dumbbell neurofibroma tumor are removed completely either by two surgeries (one from behind and one from front or side), or by a very extensive mutilating surgery which many a times require spinal fusion as well. Here we successfully tried a new key hole approach from side to completely remove the tumor in one operation without opening the spine.
New technique for removal of spinal tumour without opening up the spine in Single approach: Worldwide dumbbell neurofibroma tumor are removed completely either by two surgeries (one from behind and one from front or side), or by a very extensive mutilating surgery which many a times require spinal fusion as well. Here we successfully tried a new key hole approach from side to completely remove the tumor in one operation without opening the spine.
Craniovertebral Lesions
Fixed Atlantoaxial Dislocation (Fixed AAD): Standard treatment for this disorder is now Odontoidectomy with fusion in most of cases. We have done odontoid removal (odontoidectomy) through Microscopic Transoral, Endoscopic Transoral, and Endoscope guided Transnasal aooroaches. We do posterior fusion in all cases in same stage. Even ventilator support or tracheostomy is not needed in most of the cases even those with severe respiratory compromise.
Mobile AAD: Fusion is the gold standard and we do fusion with help of wires, cables, rod-screw, transarticular screw, Loupe etc. We restrict fusion to minimum number of spinal segments to preserve motion segment.
ACM- Syrinx: We do posterior decompression with or without duraplasty for Arnold Chiari Malfomation. Syrinx is treated by correcting defect, deformity or syringeal shunting
Odontoid fracture: Depending upon fracture type, we do transodontoid screw fixation, Posterior fusion by wires, cables, rod-screw, transarticular screw, Loupe etc. We restrict fusion to minimum no of spinal segments to preserve motion segment.
We have tried Movement-Preserving Posterior Restriction (MPPR) technique with success in one case, it preserved the atlantoaxial movements in the case
Spinal Tuberculosis
We treat all cases of spinal tuberculosis by nonsurgical as well as appropriate decompression –stabilization technique. We also do surgery for cases who had residual compression or in adequate stabilization after previous surgery. Even very old, flail patients (80 years old) have tolerated reoperation well in our centre. Most of our patient improved significantly. Almost all of our patients have achieved ambulatory state.