Spinal Injury and Degeneration
Lumbar Disc
- 1. Spontaneous resolution occurs in most cases while trying various treatments like bed rest, traction, massage , Desi treatments etc. There is no specific medicine for disc prolapsed: all medicines given are for relief of symptoms
- 2. Minimally Invasive Microdiscectomy (Endoscopic or Microscopic): Cut as small as 2-3 cm qwhich can be covered with band-aid (hence we call it Band-aid procedure). Pains less sometimes lesser than even percutaneous methods. Generally walking allowed on the day of surgery.
Though we are using endoscopic technique for more
than 8 years but feel that microscopic approach is better than endoscopic.

- 3. Percutaneous Tube discectomy (Microscopic or Endoscope- guided): We use a cut as small as 1.5 cm (as small as used anywhere in the world, if not smaller) pass a wire under guidance of C-arm. Once at right place, we pass dilators and then a tubular retractor (the structure on the way to disc are thus only pushed aside, not cut so that they come in their place after surgery). Through this tube we use endoscope or microscope for safe disc removal. We remove only that part of the disc which cause symptoms, rest of the disc is not disturbed as it is still functional. This surgery is as safe as microdiscectomy but less painful. We are doing it for 5 years and feel microscopic surgery is better than endoscopic.

- 4. Hemilaminectomy or Interlaminar aaproach for Microdiscectomy: Disc is removed through smaller (4-5 cm) ut still some avoidable destruction of spine is done. Use of Microscope makes microdiscectomy safer than open disc removal procedure. We no longer encourage it in our hospital.

- 5. Laminectomy for disc removal (Open method): Done through large cut and is more mutilating than needed.

- 6. Percutaneous Needle disc procedures (chemo/automated/endoscopic/ Hydro/LASER): Useful only for minor disc prolapsed (grade 2, where disc material does not come out of disc covering completely). It is neither good, nor safe for higher grade (grade 3-4) i.e. extruded or migrated disc (where disc material completely comes out of its covering and even may go up or down in spinal canal ). We do only endoscope guided intradiscal procedures. For LASER NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE, UK has mentioned that it was performed in very few specialist centres; had risk of damage to nerve roots, vertebral endplates and neighbouring structures, and disc space infection. Most spinal surgeons believe the procedure is ineffective. The equipment is described as expensive and requires x-ray imaging and/or percutaneous arthroscopy. A brief appraisal of all the available literature suggests that surgical failures are frequently due to the presence of free fragments, which suggests that selection criteria for patients should be carefully considered.
Lumbar Canal Stenosis
Some of the options (besides nonsurgical treatments) are Laminectomy, Laminoplasty, Unilateral approach –Sublaminar decompression
Lumbar Listhesis
Posterior fusion, ALIF, PLIF, & TLIF are the various options for fusion when adequate trial of nonsurgical treatment fails.
Cervical Disc Prolapse
Spontaneous resolution occurs in many while rest, collar, Traction etc are tried. Where it fails to resolve spontaneously or sufferings are severe or disabling, then surgical options are considered. We offer Discectomy & Fusion (Open or Microscopic or Endoscopic), Discectomy without fusion, Disc-Preserving microdiscectomy (endoscopic or Microscopic) and Disc replacement (Disc arthroplasty).
Cervical Stenosis or Spondylosis
We offer following options besides nonsurgical options
- (1) Posterior decompression with or without fusion,
- (2) Anterior decompression and Fusion
Thoracic Disc
- (1) Conventional open: Costotransversectomy/Lateral extracavitary/Thoracotomy: Needs large cut (10-12 inch) and associated significant local pain , blood loss and tissue destruction. Now we need these methods only occasionally.
- (2) Endoscopic discectomy: Avoids large cut and local pain. However, single lung ventilation increases risks of lung complications, particularly for elderly and those with respiratory problems.
- (3) Minimally Invasive Microscectomy: We do it with 3 inch or lesser cut with a technique which reduces lung related problems to large extent and in our hands, has proven to be safe for as old as 80 years old.
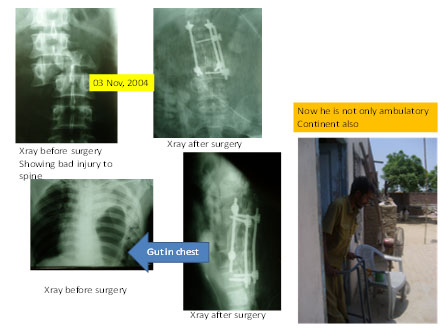
Spinal Injury/Trauma
We have been doing all types of anterior, lateral, posterior and combined approaches for all segments of spine from CV Junction to sacrum. We believe in and have tried adequate decompression of the spinal cord and nerve tissue and rigid stabilization as the gold standard of management of spinal injury. We believe that the good results we have achieved in our surgical most cases are because of this.
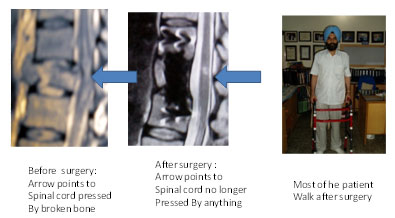
We have managed some of the worst spinal injuries with very good outcome based on same principle:
Spinal Cord Injury Without Radiological Abnormality (SCIWORA)
These patient have neurological deterioration even with minor injury. Recovery generally occurs, but which may not be optimum. The index case shown was operated after 1-2 yr of injury because he failed to recover beyond certain level. Recovery ensued after adequate decompression.
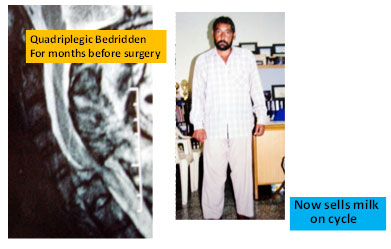
OLD spinal Injury
We have seen that certain cases of spinal cord injury can be helped by surgery even many after injury (as late as 13 years after injury). They may have significant recovery in weakness or deficit, Bedsores may heal, contractures and spasm may decrease, making care easier, simpler and life more pleasant.
Our Minimally Invasive Thoracoabdominal anterolateral approach to mid and lower thoracic and upper lumbar spine
We use smaller incision (2-3 inches in most recent cases as compared to usual12-15 inches in conventional approach) and many technical nuances perfected at our own center, which has reduced the postoperative complications and minimized the pain. We have operated more than 20 cases older than 60 years (even 80 years old)
with favourable recovery and outcome. SAFE AND EFFECTIVE.

Osteoporotic Fracture
We also do Percutaneous Vertebroplasty and Kyphoplasty with MMA in medically nonresponding patients.