Head and Spinal Injury
Simple principles and promptness saves life and quality of life in cases of head and spinal injury. We manage all cases of head and spinal injury, including
- Extradural Hematoma
- Acute and Chronic Subdural hematoma
- Subdural Hygroma
- Intracerebral contusion or hematoma
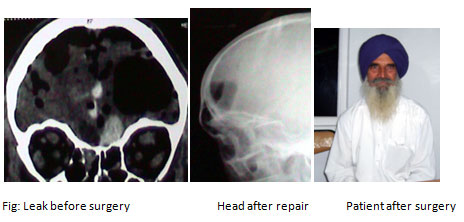
- CSF leak from nose or ear
- Penetrating brain injury
- Firearm injury
- Depressed fracture
- Diffuse axonal Injury
- Faciomaxiallry injury
- Spinal fracture and dislocations
- Traumatic disc prolapsed
- SCIWORA (spinal cord injury without radiological abnormality)
- Old spinal cord injury
- Craniotomy bone flap defect
- Posttraumatic syrinx
- Posttraumatic spinal deformity
No case is bad enough to be rejected as “gone case.” We have cases who have improved to independent working status after prompt surgery, even after they had tentorial herniation (an ominous stage). All decisions are taken by the neurosurgeon themselves without intervening other specialist, saving time and giving better results
CSF rhinorrhoea (watery fluid leak from nose after head injury or without injury)
Our options (besides nonsurgical) are Conventional Microsurgical approach for Basal repair Microsurgical unilateral approach (Preserves smell sensibility of other side)
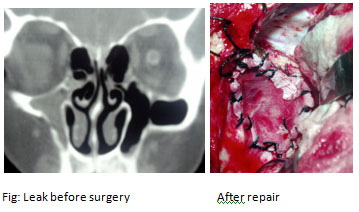
Endoscopic approach: which may preserve smell sensation and avoids any external cut